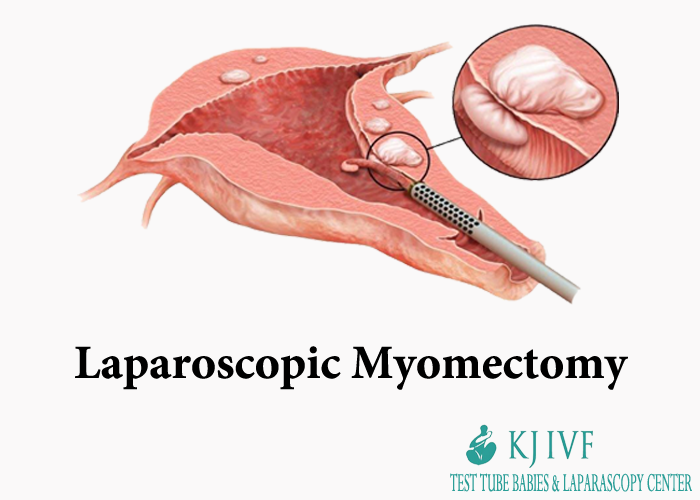
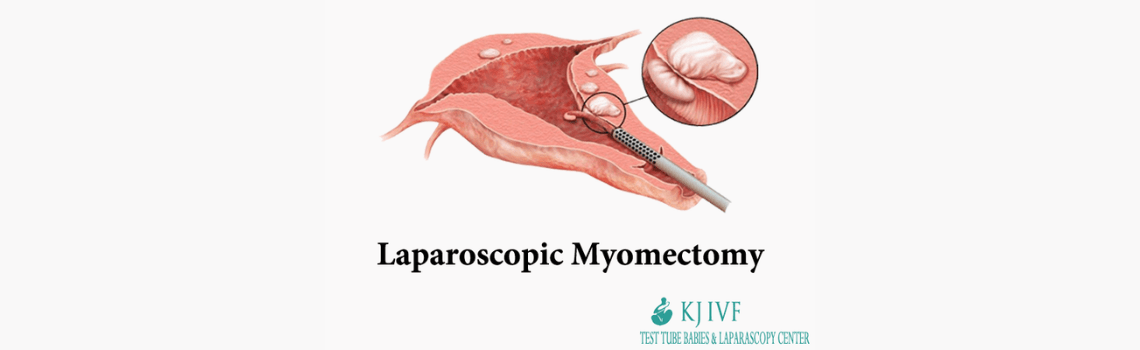
Laparoscopic Myomectomy
Myomectomy is a surgical procedure to remove fibroids from uterus. Fibroids are common noncancerous tumors that appear in the uterus.
Myomectomy can be done through abdominal route, Laparoscopically or Hysteroscopically depending on size and position of fibroids. Laparoscopic Myomectomy is performing myomectomy through key hole incision.
The goal of surgery during myomectomy is to take out symptom-causing fibroids and reconstitute the uterus. Unlike a hysterectomy, which removes the entire uterus, a myomectomy removes only the fibroids and leaves your uterus.
INDICATIONS OF MYOMECTOMY
Your doctor might advise myomectomy for fibroids causing symptoms that are troublesome. If you need surgery, reasons to choose a myomectomy over a hysterectomy for uterine fibroids include:
- You want to bear children
- Your doctor suspects fibroids might be interfering with your fertility
- You want to retain your uterus
TYPES OF MYOMECTOMY
Several surgical techniques are used to remove the fibroid from the uterus. The choice of the technique depends on various factors such as the position and size of the fibroids as well as the characteristics of the patient. Various types of Myomectomy are as described under –
-
Laparoscopic Myomectomy is a procedure to remove the fibroids present in the uterus. This technique is performed using a narrow telescope like an instrument used to see inside the abdomen. The procedure involves small 3 to 4 incisions in the navel and lower abdomen. Fibroids are enucleated from the uterus repairing the uterus incision. Recovery time is around 2 to 3 weeks and requires one night of the hospitalization. Complications such as the bleeding, injury to internal organs, an infection might occur during this procedure which is minimal.
-
Abdominal Myomectomy, is performed using a horizontal or vertical incision in the abdominal wall. It enables the surgeon to have direct access to the patient’s uterus and usage of traditional surgical techniques and instruments is done. Anesthesia is given to the patient and a full recovery is expected within the 4 to 6 weeks.
-
Hysteroscopic Myomectomy allows removing a submucosal fibroid from the inside wall of the uterus. A narrow telescope-like instrument is passed through the vaginal route to visualize the uterine cavity in order to allow surgery inside the uterus. This procedure is only performed for the smaller fibroid. This procedure is performed under the anesthesia in an operating room. Some of the complication faced during this procedure includes fluid overload, bleeding, the formation of the scarring inside the uterus, and uterine perforation.
HOW IS LAPAROSCOPIC MYOMECTOMY PERFORMED?
The procedure is performed under the anesthesia. The operating surgeon makes four small incisions. These incisions are of about half an inch long each into the lower abdomen. The abdomen is filled with carbon dioxide gas so that the surgeon can see inside the abdomen. A laparoscope is placed into one of the incisions by the surgeon. A laparoscope is basically a illuminated narrow tube with the camera attached on one end. On the other incision, the small instruments are placed.
To remove the fibroids from the uterus, the surgeon will cut the fibroids into the small pieces. The fibroids are pushed out of the vagina or through the small openings into the abdomen. Once the fibroids are removed, the surgeon will reshuffle the instruments, release the gas and close the incisions. If the fibroids are too big, abdominal Myomectomy Treatment is used where a large incision is made in the abdomen to remove the fibroids.
WHAT IS THE DURATION OF SURGERY FOR LAPAROSCOPIC MYOMECTOMY ?
Again, depending on the size, site and number of fibroids the duration of surgery can vary from few minutes to a couple of hours.
AFTER THE PROCEDURE OF LAPAROSCOPIC MYOMECTOMY
Patient usually has to stay for around a day in the hospital after the procedure is done. Usually, doctors prescribe oral pain relief medications after the surgery and give instruction on the diet and activities. Women can expect staining and vaginal spotting for a couple of days up to six weeks depending on the type of procedure done.
Laparoscopic Myomectomy is a less invasive procedure in which women have less pain, lose less blood, and can return to the normal activity more quickly as compared to other treatments such as laparotomy.
BENEFITS OF LAPAROSCOPIC MYOMECTOMY
Compared to other types of myomectomy, Laparoscopic Myomectomy is considered as an effective and safe procedure to remove fibroids from the uterus. Some of the benefits are as follows –
- It causes less loss of blood during the procedure.
- This type of treatment does not take a long time and the patient gets a discharge within a day.
- Postoperative recovery is quicker
RISKS OF LAPAROSCOPIC MYOMECTOMY
Laparoscopic Myomectomy has the low complication rate. Still, the procedure poses a unique set of the challenges. Risks include:
-
Excessive Blood Loss – Many women with uterine fibroids already have low hemoglobin (anemia) due to heavy bleeding during periods, so they’re at a higher risk of complications due to blood loss. Your doctor may suggest ways to build up your hemoglobin before surgery.
During the procedure surgeons take extra measures to avoid excessive bleeding. These may include blocking blood flow from the uterine blood vessels by tourniquets and clamps and injecting medications around fibroids to cause blood vessels to constrict. However, most steps don’t decrease the risk of needing a transfusion.
In General, Studies Suggest that there is Less Blood Loss with the Hysterectomy than Myomectomy for Similarly Sized Uteruses.
-
Scar Tissue – Surgical incisions in the uterus to remove fibroids can lead to adhesions — bands of scar tissue that may develop post surgery. Laparoscopic Myomectomy may result in the fewer adhesions than abdominal myomectomy (laparotomy).
-
Pregnancy Women who have undergone – myomectomy have certain risks during delivery if they become pregnant. If your operating surgeon had to make a deeper incision in your uterine wall, the gynecologist who manages your subsequent pregnancy may recommend cesarean delivery (C-section) to avoid rupture of the uterus during labor, a very rare complication of pregnancy and labor. Fibroids themselves are also associated with the pregnancy complications.
-
Rare Chance of Hysterectomy – Rarely, in case of uncontrolled bleeding, the surgeon must remove the uterus if bleeding is uncontrollable.
-
Rare Chance of Spreading a Cancerous Tumor – Rarely, a cancerous tumor can be misdiagnosed for a fibroid. Taking out the tumor, especially if it’s broken into the little pieces (morcellation) to remove through a small incision, can lead to spread of the cancer. The risk of this happening increases after the menopause and as women age.
MEASURES TO PREVENT SURGICAL COMPLICATIONS
To minimize risks of myomectomy surgery, your surgeon may recommend:
-
Iron Supplements and Vitamins – If you have anemia from heavy menstrual periods, your doctor might recommend iron supplements and vitamins to allow you to build up your haemoglobins before surgery.
-
Hormonal Treatment – Another way to correct anaemia is hormonal treatment before surgery. Your doctor may prescribe a gonadotropin-releasing hormone (GnRH) agonist, oral birth control pill or other hormonal medications to stop or decrease your menstrual flows.
-
Therapy to Shrink Fibroids – Some hormonal treatment, such as GnRH agonist therapy, can also shrink your fibroids and uterus enough to allow your surgeon to use a minimally invasive surgical approach — such as a smaller, horizontal incision rather than a vertical incision, or a laparoscopic procedure instead of an open procedure.
In most patients, GnRH agonist treatment causes symptoms of menopause, including hot flashes, night sweats and vaginal dryness. However, these discomforts vanish after you stop taking the medication. Treatment generally takes place — over several months before surgery.
Evidence suggests that not all patients should take GnRH agonist treatment before myomectomy. GnRH agonist treatment may soften and shrink fibroids so much that their detection during surgery becomes more difficult.
Another class of drugs called selective progesterone receptor modulators (SPRMs), such as ulipristal, may also shrink fibroids and reduce the bleeding. Outside the United States, ulipristal is approved for three months of therapy before the myomectomy.
HOW TO PREPARE BEFORE LAPAROSCOPIC MYOMECTOMY
Patient needs overnight fast i.e. stop drinking fluids and eat anything in the night before the surgery. Surgeon’s instructions must be followed before the surgery. In case if the patient is already on any type of medication, it is preferable to consult the doctor to continue with the medication or not.
General anesthesia is used for the laparoscopic, robotic, abdominal, and certain hysteroscopic myomectomy in which the patient is fast asleep during the procedure. Spinal anesthesia is used for the certain hysteroscopic myomectomies in which the patient is injected in the spinal canal to anaesthetise the nerves in the lower half of the body.
AFTER THE PROCEDURE
At discharge from the hospital, your doctor prescribes oral pain medication, tells you how to care for yourself, and discusses restrictions on your diet and the activities. You can expect some vaginal spotting or staining for a few days up to the six weeks, depending on the type of procedure you’ve had.
RESULTS OF LAPAROSCOPIC MYOMECTOMY
Following outcomes are possible after myomectomy:
-
Symptomatic Relief – After myomectomy, most women experience relief of bothersome signs and symptoms, such as heavy menstrual bleeding and pelvic pain and pressure.
-
Fertility Improvement – Women who undergo laparoscopic myomectomy, with or without robotic assistance, have good chances of achieving pregnancy within about a year of surgery. After a myomectomy, the suggested waiting time is three to six months before attempting pregnancy to allow your uterus time to heal.
Fibroids that your surgeon didn’t detect during surgery or fibroids that are incompletely removed could eventually grow and cause symptoms. New fibroids, which may or may not require the treatment, can also develop. Patients who had only one fibroid have the lower risk of developing new fibroids — often termed the recurrence rate — than do patients who had multiple fibroids.
WHY KJIVF FOR LAPAROSCOPIC MYOMECTOMY?
- First full-fledged Laparoscopy and IVF Center of Delhi, India – 21 years of quality care.
- Premium and only teaching the ART center of East Delhi, Delhi NCR, Faridabad, India.
- Results and the success rates at par with the Best in the world.
- Affordable compared with the rest, we have reasonable costs & pricing of all laparoscopic procedures.
- Complete transparency is our key concern and thorough counseling to help you decide the right treatments.
- Highly trained consultants.
- Ethical practice/No false claims.
- Individualized care and treatment.
- All basic and advanced facilities under one roof.
- Individual protocols to make the whole treatment affordable and cost-effective.
- Advanced IVF: ICSI, PESA/TESA, PICSI, blastocyst culture, egg/ sperm donation program, and vitrification, etc. are all available.
For more queries, Call us at +919650725386, +91 011 3560 4368.
Our Related Searches:-
Laparoscopic Myomectomy in Delhi
Laparoscopic Myomectomy in Faridabad
Laparoscopic Myomectomy in India
Laparoscopic Myomectomies Doctors In Delhi
Laparoscopic Myomectomies Doctors In Faridabad
Laparoscopic Myomectomies Doctors In India
Laparoscopic Myomectomy Cost in Delhi
Laparoscopic Myomectomy Cost in Faridabad
Laparoscopic Myomectomy Cost in India
Laparoscopic Myomectomy Treatment in Delhi
Laparoscopic Myomectomy Treatment in Faridabad
Laparoscopic Myomectomy Treatment in India
Laparoscopic Myomectomy Surgery in Delhi
Laparoscopic Myomectomy Surgery in Faridabad
Laparoscopic Myomectomy Surgery in India